
16% Indian Women Don’t Get Pregnancy Care--Nearly Half Because Husband/Family Did Not Think It Necessary

Chennai: More than one in seven Indian women did not receive antenatal care during their last pregnancy--nearly half of them because their husband or family did not think it was necessary or did not allow it--according to the latest National Family Health Survey 2015-16 (NFHS-4) data, highlighting the need to sensitise men about women’s rights to healthcare.
Antenatal care (ANC) constitutes healthcare for pregnant women to monitor for signs of complications, detect and treat hypertension and diabetes, provide iron and folic acid tablets and counsel on preventive care, diet during pregnancy, delivery care, postnatal care etc. ANC is provided by a skilled healthcare provider such as a doctor, auxiliary nurse midwife (ANM) or other health professionals.
Only 16.7% women in rural India received full antenatal care--at least four ANC visits, at least one tetanus toxoid injection, and iron and folic acid tablets or syrup taken for 100 or more days--about half as many as in urban areas (31.1%), NFHS-4 data show.
The World Health Organization recommends that all pregnant women receive at least four ANC visits, and that the first such visit should be in the first trimester of pregnancy.
The gendered nature of decision-making in Indian households also affects women’s healthcare seeking behaviour.
26% men did not think pregnancy care was necessary/did not allow it
One in four men whose wives did not receive ANC said they did not think it was necessary. One in five men said their family members did not think it was necessary while one in ten said the women themselves thought ANC to be unnecessary. Nearly one in four men said it was ‘too costly’.
Note: This data is from men’s report
A larger share of urban men and their families were more likely to think ANC was not necessary or to not permit the ANC, data show.
While this is intriguing and needs further study, a smaller proportion of deliveries in urban areas were in public facilities (46.2%) compared to rural areas (54.4%), suggesting that private health facilities may not be providing the right kind of pregnancy-related advice to couples.
Only 14.7% women in urban India were in the labourforce, compared to 24.8% in rural india, according to the National Sample Survey Office’s Employment Unemployment Survey, 2011-12, thus reducing their access to income, and thereby independence in decision-making.
More rural men cited financial reasons for their wives not receiving ANC.
The gendered nature of household decision-making, as we said, also affects women’s healthcare seeking behaviour. Only 12% women said they made decisions related to their health on their own, while 22.6% said their husband made the decisions and 62.5% said they made the decision jointly with their husbands.
The percentage of women who made decisions related to their health fell 15.1 percentage points between 2005-06 and 2015-16.
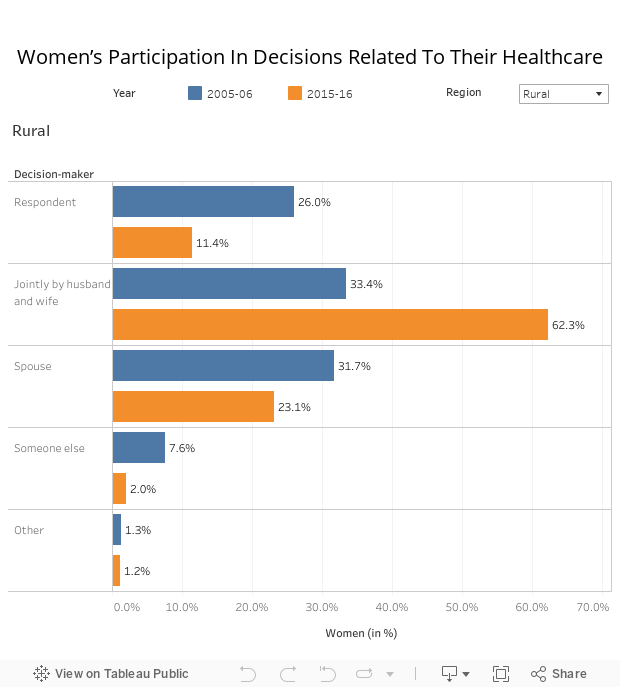
Source: National Family Health Survey, 2015-16
Improved levels of educational attainment, participating in income-generating employment and belonging to households in the higher wealth quintiles tend to raise women’s participation in decision-making about their own health, data show.
Even as India’s female labour force participation is declining--as IndiaSpend is investigating in an ongoing series--only one-fifth of women who worked decided how their earnings should be used, illustrating the need to improve women’s agency in household decision-making.
Few men informed on what to do in case of pregnancy complications
In 2015-16, among women who received an ANC visit, nearly seven in 10 husbands were present during at least one ANC visit--up 18.7 percentage points from 49.5% in 2005-06. Urban areas fared better: 76.9% men were present for the ANC visit compared to 63.9% in rural areas.
More educated men and men from the highest quintile of household wealth were more likely to be present during their wife’s ANC visit, data show.
Of men who were present during ANC, only 38.6% were told of complications such as convulsions, 37.1% were told of vaginal bleeding, 45.2% were told of prolonged labour, 44.8% were told of high blood pressure and 51.1% were told of severe abdominal pain. Also, only 47.1% of men were counselled by health providers on the course of action to be taken if their wife developed a pregnancy-related complication.
So, men end up participating in decisions about their spouse’s health without adequate knowledge, which could delay health seeking.
A large number of maternal and child deaths are attributable to the delay in deciding to seek care, reaching the appropriate health facility, and receiving quality care once inside an institution, according to this 2013 document from India’s health and family welfare ministry.
Why antenatal care is crucial
Only 30.3% Indian women consumed iron and folic acid tablets for the recommended course of 100 days or more. Consequently, 50.3% pregnant women and 58.4% of children aged 6-59 months had iron-deficiency anaemia--a major cause of maternal deaths, preterm births and mortality of infants.
India’s infant mortality rate is 34 deaths per 1,000 live births--the highest among BRICS countries. The neonatal mortality rate in India was 25 per 1000 live births and under five mortality rate was 43 per 1,000 live births in 2015 shows data from Sample Registration System Statistical Report 2015.
Further, India’s maternal mortality ratio of 167 deaths per 100,000 live births in 2011-13 was also the worst among BRICS nations.
Post-delivery, only 41.5% of infants were breastfed within an hour of birth and the median duration of exclusive breastfeeding was 2.9 months. Further, less than 10% of infants aged 6-23 months were given a minimum acceptable diet, data from NFHS-4 show.
These sub optimal feeding practices along with poor sanitation and other social determinants result in a stunting (low height for age) prevalence of 38.4% and underweight (low weight for height) prevalence of 35.7% among children under five years.
Besides improving infrastructure and human resources in healthcare, policy attention to promote women’s agency through education and paid employment as well as sensitising men about women’s right to healthcare and providing information to them on maternal and child healthcare is crucial to achieve the related sustainable development goal targets.
(Gayathri Balagopal is a Chennai-based independent researcher.)
We welcome feedback. Please write to respond@www.health-check.in. We reserve the right to edit responses for language and grammar.
