
100% Wrong: Rural Medical Staff Make Diarrhoea Life-Threatening

More than 90% of treatments for childhood diarrhoea and pneumonia--the leading causes of death among Indian children--are incorrect, a new study has said. Instead, largely unqualified medical practitioners, unfamiliar with relatively simple life-saving medications, prescribe antibiotics and other potentially harmful drugs, said the study, published recently in JAMA Pediatrics (JAMA stands for Journal of the American Medical Association). “Only 20% of the providers in our sample had medical qualifications," said Manoj Mohanan, lead author and professor at Duke University's Sanford School of Public Policy in an interview with IndiaSpend. "However, it is also important to note that this is not unusual in rural settings." The results indicate that India's strategies to reduce child mortality rates--among the world's highest--need to be reassessed and modified. Among 15 high-burden countries, India ranks third from bottom for its use of life-saving intervention for children at risk of dying from diarrhoea and pneumonia, this 2014 study noted. The number of children under five dying from diarrhoea and pneumonia was the highest, with 318,000 deaths in 2013. The Duke study involved 340 healthcare providers in Bihar, which has India's highest mortality rate for children between one and four years of age: 55 die for every 1,000 live births. Child mortality in India has declined 55% over the past 24 years, as IndiaSpend previously reported, but too many still die. India lags the majority of the world's countries (see chart), including poorer neighbours Bangladesh and Nepal. 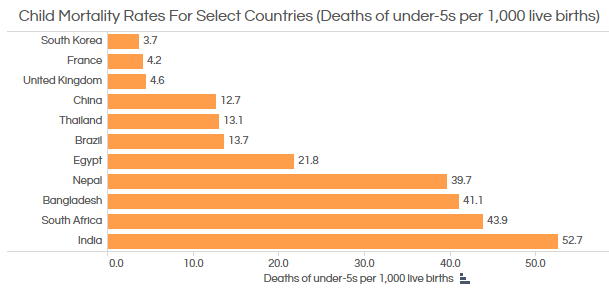 Source: World Bank Researchers conducting the study assessed practitioners through what are called "standardised patients" and "vignettes". Vignette interviews assess how practitioners would treat a hypothetical case. Standardised patients, people who come as patients with the same symptoms used in the vignettes, later made incognito visits to the practitioners. This approach allowed a measurement of what is known as the "know-do gap", the difference between what practitioners know and what they do. The know-do gap appears substantial. Whether trained or not, medical practitioners examined in the study fared badly in interviews and worse in practice (see chart below).
Source: World Bank Researchers conducting the study assessed practitioners through what are called "standardised patients" and "vignettes". Vignette interviews assess how practitioners would treat a hypothetical case. Standardised patients, people who come as patients with the same symptoms used in the vignettes, later made incognito visits to the practitioners. This approach allowed a measurement of what is known as the "know-do gap", the difference between what practitioners know and what they do. The know-do gap appears substantial. Whether trained or not, medical practitioners examined in the study fared badly in interviews and worse in practice (see chart below). 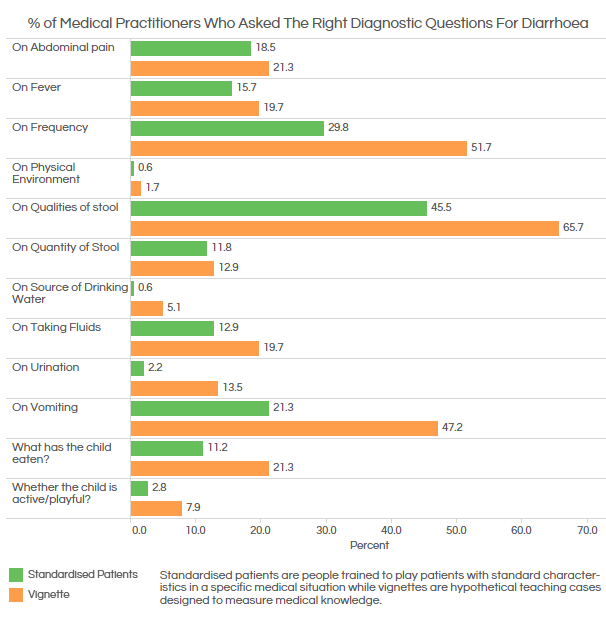 Source: JAMA Pediatrics "Less than 10% of practitioners [see chart below] prescribed the correct treatment and referral for cases of watery diarrhoea and pneumonia, and inappropriate and potentially dangerous medications were prescribed for a significant proportion of the standardised patients," noted an accompanying editorial in JAMA Pediatrics, written by James Tielsch, chair of the Department of Global Health at George Washington University.
Source: JAMA Pediatrics "Less than 10% of practitioners [see chart below] prescribed the correct treatment and referral for cases of watery diarrhoea and pneumonia, and inappropriate and potentially dangerous medications were prescribed for a significant proportion of the standardised patients," noted an accompanying editorial in JAMA Pediatrics, written by James Tielsch, chair of the Department of Global Health at George Washington University. 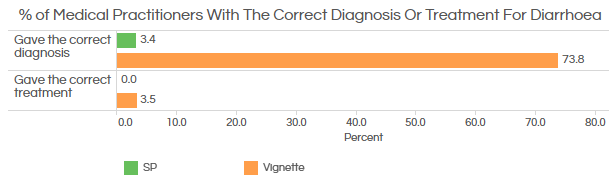 Source: JAMA Pediatrics "For simple diarrhoea, where the only treatment necessary was ORS (oral rehydration salts) and zinc without any antibiotics or other harmful drugs, [none of the] providers gave the right treatment," said Mohanan. None of the dummy patients asked for antibiotics or other drugs. Only 17% of practitioners prescribed (ORS), a low-cost, easily available and effective treatment, although 72% said they would use ORS--but obviously did not. Practitioners who did give ORS, also prescribed harmful or unnecessary drugs, such as antibiotics (see chart below), resistance to which is spreading across India and putting millions at risk, as IndiaSpend has reported.
Source: JAMA Pediatrics "For simple diarrhoea, where the only treatment necessary was ORS (oral rehydration salts) and zinc without any antibiotics or other harmful drugs, [none of the] providers gave the right treatment," said Mohanan. None of the dummy patients asked for antibiotics or other drugs. Only 17% of practitioners prescribed (ORS), a low-cost, easily available and effective treatment, although 72% said they would use ORS--but obviously did not. Practitioners who did give ORS, also prescribed harmful or unnecessary drugs, such as antibiotics (see chart below), resistance to which is spreading across India and putting millions at risk, as IndiaSpend has reported.  Source: JAMA Pediatrics So why do so many providers prescribe antibiotics? That is unclear. "Why they prescribe antibiotics when they know this is not clinically appropriate, is a tough question." said Mohanan. "We are currently studying precisely this issue in follow-up studies. Part of the explanation could be that a lot of them earn money from selling drugs (plausibly because of a missing market for medical consultations in rural settings, where patients might be willing to pay for a ‘treatment’ but not for medical advice)." Other factors in over-prescribing antibiotics could be that providers underestimate the emergence of drug resistance, long-term adverse effects on patients or simply believe that guidelines on antibiotic use somehow do not apply to local conditions. "Hopefully we’ll have more empirical evidence on this in coming years," said Mohanan. Since the study was done in Bihar, are its findings applicable across India? "Our previous studies using standardised patients collected data from urban Delhi and rural Madhya Pradesh, and the patterns in quality of care were very comparable," said Mohanan. "I cannot say it is generalisable across all parts of the country, but it is plausible that our findings are generalisable to rural India, where most healthcare is provided by untrained practitioners." Tielsch wrote that the study was "a stark reminder that there remains a large, difficult-to-address, unfinished agenda for child health and survival in under-served populations around the world". "Better understanding of how comprehensive strategies to address the know, do, and quality gaps across a range of practice environments is needed to prepare for the ambitious upcoming sustainable-development goals that call for elimination of preventable mortality among women and children." (Samar Halarnkar is the Editor of IndiaSpend.com) _____________________________________________________________ “Liked this story? Indiaspend.org is a non-profit, and we depend on readers like you to drive our public-interest journalism efforts. Donate Rs 500; Rs 1,000, Rs 2,000.”
Source: JAMA Pediatrics So why do so many providers prescribe antibiotics? That is unclear. "Why they prescribe antibiotics when they know this is not clinically appropriate, is a tough question." said Mohanan. "We are currently studying precisely this issue in follow-up studies. Part of the explanation could be that a lot of them earn money from selling drugs (plausibly because of a missing market for medical consultations in rural settings, where patients might be willing to pay for a ‘treatment’ but not for medical advice)." Other factors in over-prescribing antibiotics could be that providers underestimate the emergence of drug resistance, long-term adverse effects on patients or simply believe that guidelines on antibiotic use somehow do not apply to local conditions. "Hopefully we’ll have more empirical evidence on this in coming years," said Mohanan. Since the study was done in Bihar, are its findings applicable across India? "Our previous studies using standardised patients collected data from urban Delhi and rural Madhya Pradesh, and the patterns in quality of care were very comparable," said Mohanan. "I cannot say it is generalisable across all parts of the country, but it is plausible that our findings are generalisable to rural India, where most healthcare is provided by untrained practitioners." Tielsch wrote that the study was "a stark reminder that there remains a large, difficult-to-address, unfinished agenda for child health and survival in under-served populations around the world". "Better understanding of how comprehensive strategies to address the know, do, and quality gaps across a range of practice environments is needed to prepare for the ambitious upcoming sustainable-development goals that call for elimination of preventable mortality among women and children." (Samar Halarnkar is the Editor of IndiaSpend.com) _____________________________________________________________ “Liked this story? Indiaspend.org is a non-profit, and we depend on readers like you to drive our public-interest journalism efforts. Donate Rs 500; Rs 1,000, Rs 2,000.”
Source: World Bank Researchers conducting the study assessed practitioners through what are called "standardised patients" and "vignettes". Vignette interviews assess how practitioners would treat a hypothetical case. Standardised patients, people who come as patients with the same symptoms used in the vignettes, later made incognito visits to the practitioners. This approach allowed a measurement of what is known as the "know-do gap", the difference between what practitioners know and what they do. The know-do gap appears substantial. Whether trained or not, medical practitioners examined in the study fared badly in interviews and worse in practice (see chart below). Source: JAMA Pediatrics "Less than 10% of practitioners [see chart below] prescribed the correct treatment and referral for cases of watery diarrhoea and pneumonia, and inappropriate and potentially dangerous medications were prescribed for a significant proportion of the standardised patients," noted an accompanying editorial in JAMA Pediatrics, written by James Tielsch, chair of the Department of Global Health at George Washington University. Source: JAMA Pediatrics "For simple diarrhoea, where the only treatment necessary was ORS (oral rehydration salts) and zinc without any antibiotics or other harmful drugs, [none of the] providers gave the right treatment," said Mohanan. None of the dummy patients asked for antibiotics or other drugs. Only 17% of practitioners prescribed (ORS), a low-cost, easily available and effective treatment, although 72% said they would use ORS--but obviously did not. Practitioners who did give ORS, also prescribed harmful or unnecessary drugs, such as antibiotics (see chart below), resistance to which is spreading across India and putting millions at risk, as IndiaSpend has reported. Source: JAMA Pediatrics So why do so many providers prescribe antibiotics? That is unclear. "Why they prescribe antibiotics when they know this is not clinically appropriate, is a tough question." said Mohanan. "We are currently studying precisely this issue in follow-up studies. Part of the explanation could be that a lot of them earn money from selling drugs (plausibly because of a missing market for medical consultations in rural settings, where patients might be willing to pay for a ‘treatment’ but not for medical advice)." Other factors in over-prescribing antibiotics could be that providers underestimate the emergence of drug resistance, long-term adverse effects on patients or simply believe that guidelines on antibiotic use somehow do not apply to local conditions. "Hopefully we’ll have more empirical evidence on this in coming years," said Mohanan. Since the study was done in Bihar, are its findings applicable across India? "Our previous studies using standardised patients collected data from urban Delhi and rural Madhya Pradesh, and the patterns in quality of care were very comparable," said Mohanan. "I cannot say it is generalisable across all parts of the country, but it is plausible that our findings are generalisable to rural India, where most healthcare is provided by untrained practitioners." Tielsch wrote that the study was "a stark reminder that there remains a large, difficult-to-address, unfinished agenda for child health and survival in under-served populations around the world". "Better understanding of how comprehensive strategies to address the know, do, and quality gaps across a range of practice environments is needed to prepare for the ambitious upcoming sustainable-development goals that call for elimination of preventable mortality among women and children." (Samar Halarnkar is the Editor of IndiaSpend.com) _____________________________________________________________ “Liked this story? Indiaspend.org is a non-profit, and we depend on readers like you to drive our public-interest journalism efforts. Donate Rs 500; Rs 1,000, Rs 2,000.”
Next Story